GLOMERULAR DISEASE DIAGNOSIS
FSGS: A Clinicopathological Correlation and Case-Based Approach Toward the Correct Diagnosis
In this session of Nephropathology Essentials, Dr. Rennke presented a case-based approach to FSGS. Our Moderator’s Notes are derived from his live presentation


By Dr. Pravir Baxi
Key points:
- Podocyte (visceral epithelial cell) injury is the hallmark of proteinuria
- Diffuse podocytopathy typically manifests as nephrotic syndrome with edema, hypoalbuminemia, and nephrotic range proteinuria
- Focal podocytopathy typically results in modest amount of proteinuria without overt nephrotic syndrome features
- Important to further differentiate from acquired and genetic causes
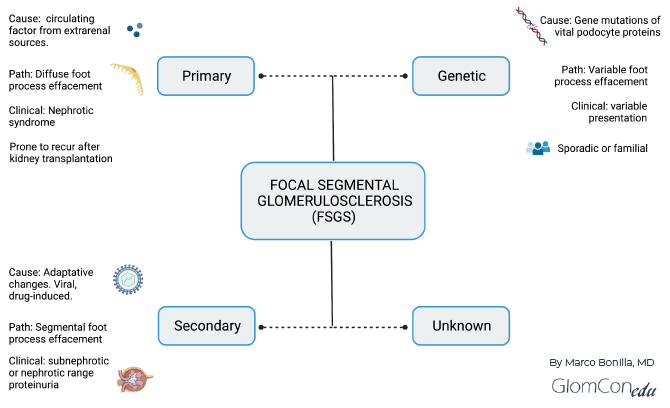
- Dr. Rennke shared his approach to the differential diagnosis of FSGS pattern of injury:
- Idiopathic or Primary FSGS
- Etiology –“Permeability Factor”
- Sudden onset of nephrotic syndrome
- Pathological Characteristics
- Normal-sized glomeruli, diffuse effacement of foot process, no significant chronicity
- Familial and Genetic FSGS
- Genetic Podocytopathies with focal Injury
- Include ACTN4 (alpha-actinin-4), TRPC6 (canonical transient receptor potential 6), INF2 (formin family of actin-regulating proteins), APOL1 mutations
- Genetic Podocytopathies with Diffuse Injury
- Include NPHS2 (podocin), NPHS1 (nephrin), PLC31 (phospholipase C epsilon), WT1 (Wilms tumor gene) mutations
- Genetic Podocytopathies with focal Injury
- Secondary or Adaptive FSGS
- The initial loss of functioning nephrons followed by adaptations
- Examples: Unilateral renal agenesis, segmental hypoplasia, and oligomeganephronie, reflux nephropathy, primary glomerulopathies, partial cortical necrosis, sickle cell disease, atheroembolic disease, cystic disease
- Without an initial loss of nephrons but with functional maladaptation
- Diabetic Nephropathy, Obesity-associated, Glycogen storage disease
- Slowly progressive proteinuria without edema, typically hx of prior kidney disease
- Pathological Features
- Glomerular hypertrophy
- Focal foot process effacement (primarily preserved)
- The initial loss of functioning nephrons followed by adaptations
- Segmental Glomerular Scarring
- Idiopathic or Primary FSGS
- Selected References:Rosenberg AZ, Kopp JB. Focal Segmental Glomerulosclerosis. Clin J Am Soc Nephrol. 2017 https://www.ncbi.nlm.nih.gov/pubmed/28242845D’Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011 https://www.ncbi.nlm.nih.gov/pubmed/22187987
Fogo AB. Causes and pathogenesis of focal segmental glomerulosclerosis. Nat Rev Nephrol. 2015 https://www.ncbi.nlm.nih.gov/pubmed/25447132
{kind=link}