DIAGNOSTIC WORKUP
Urine Microscopy with
Dr. Florian Buchkremer
Dr. Florian Buchkremer
Acknowledgment: Based on GlomCon’s Glomerular Disease Virtual Fellowship seminar “Urine Microscopy” by Dr. Florian Buchkremer.


Dr. Jian Cheng
Nephrologist
Orange Base Hospital
Australia
Urinary Sediment – The liquid biopsy of the kidney
- Method
- Centrifuge 10mL fresh urine (within 2 hours of collection) for 5 minutes at 1500rpm
- Remove 9.5mL of overlying supernatant
- Resuspend remaining urine (0.5mL)
- Pipette one drop onto slide then place a coverslip
- Examine
- Phase-contrast highlights edges e.g. of hyaline casts, and dysmorphic RBCs
- If bright field microscopy used, stains are required.
- Start at low magnification (10x) then increase the magnification (40x) after identifying areas of interest
- Phase-contrast highlights edges e.g. of hyaline casts, and dysmorphic RBCs
- @swissnephro’s approach to the analysis of the urinary sediment
- Glomerular
- Haematuria
- Dysmorphic RBCs
- RBC casts
- Proteinuria
- Lipid droplets
- Lipid casts
- Oval fat bodies
- Cholesterol plates
- Waxy casts
- Tubulointerstitial
- Tubular cell injury
- Renal tubular epithelial cells
- Renal tubular cell casts
- Granular casts
- Inflammation
- Leucocytes
- Leucocyte casts
- Waxy casts
- Crystals
- Tubular cell injury
- Urinary tract
- Non-dysmorphic RBCs
- Leucocytes
- Glomerular
Diagnostic Utility of Dysmorphic RBCs
- Pathogenesis
- Physical trauma as RBCs pass through the GBM and tubules
- Osmotic trauma as RBCs pass through the different nephron segments
- Dysmorphic RBC types to look out for:
- Acanthocytes (Mickey mouse ears) are most specific for GN
- Ringforms – These have a hole in the center
- Destructed dysmorphic RBCs – In borderline cases
- Diagnosis
- @swissnephro’s approach: If there are over >5 RBCs/hpf then assess for dysmorphic RBCs to confirm glomerular haematuria by the criteria:
- Acanthocytes >5% of RBCs or
- Acanthocytes + ringforms >30% of RBCs
- In borderline cases, include destructed dysmorphic RBCs as a clue for glomerular haematuria
- To distinguish glomerular from non-glomerular haematuria, look for other signs of glomerular injury e.g. macrophages, proteinuria, lipiduria, RBC casts
- @swissnephro’s approach: If there are over >5 RBCs/hpf then assess for dysmorphic RBCs to confirm glomerular haematuria by the criteria:
Automated vs manual urine microscopy
| Advantages of automated microscopy | Advantages of manual microscopy |
|---|---|
| Much quicker (>100 samples/h) but as good as manual microscopy in classifying RBC, WBC, and epithelial cells | More sensitive than automated microscopy for casts and crystals |
| Better in quantification (e.g. quantifying no. of RBCs as a marker in IgA nephropathy) | Better in qualification (e.g. differentiating dysmorphic from isomorphic RBCs) |
| High specificity for casts (low sensitivity, however) |
Urine Microscopy in AKI

Hyaline casts
Indicates hypovolaemia. These do not have any granules but have a smooth matrix.
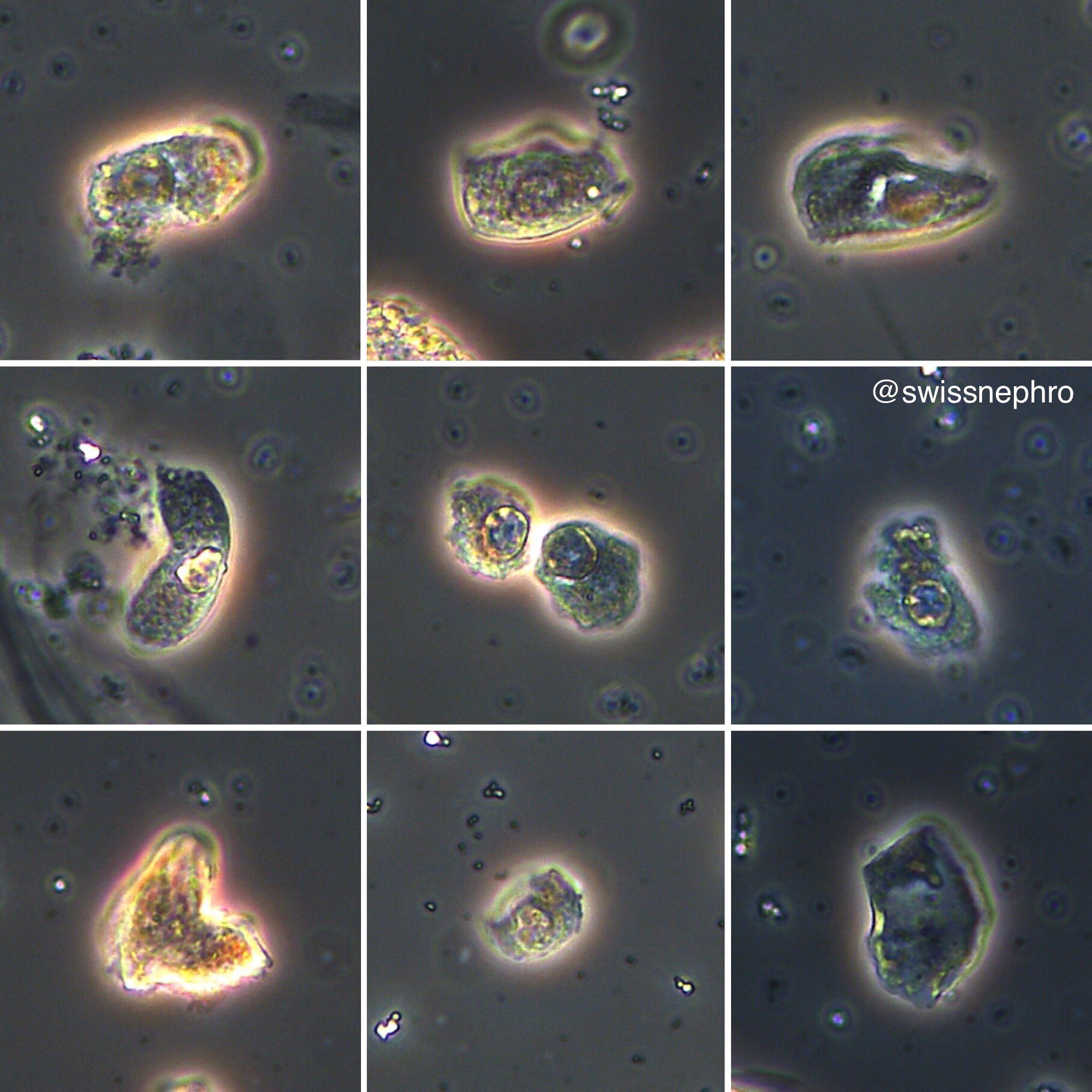
Renal tubular epithelial cells (RTECS)
Indicate ischaemic or toxic injury. Are half the size of an RBC, with a high nucleolar to cell ratio. The main differential is uroepithelial cells. Therefore, look at the company these cells keep. Granular casts, proteinuria, and an increasing creatinine suggests RTECs rather than uroepithelium.
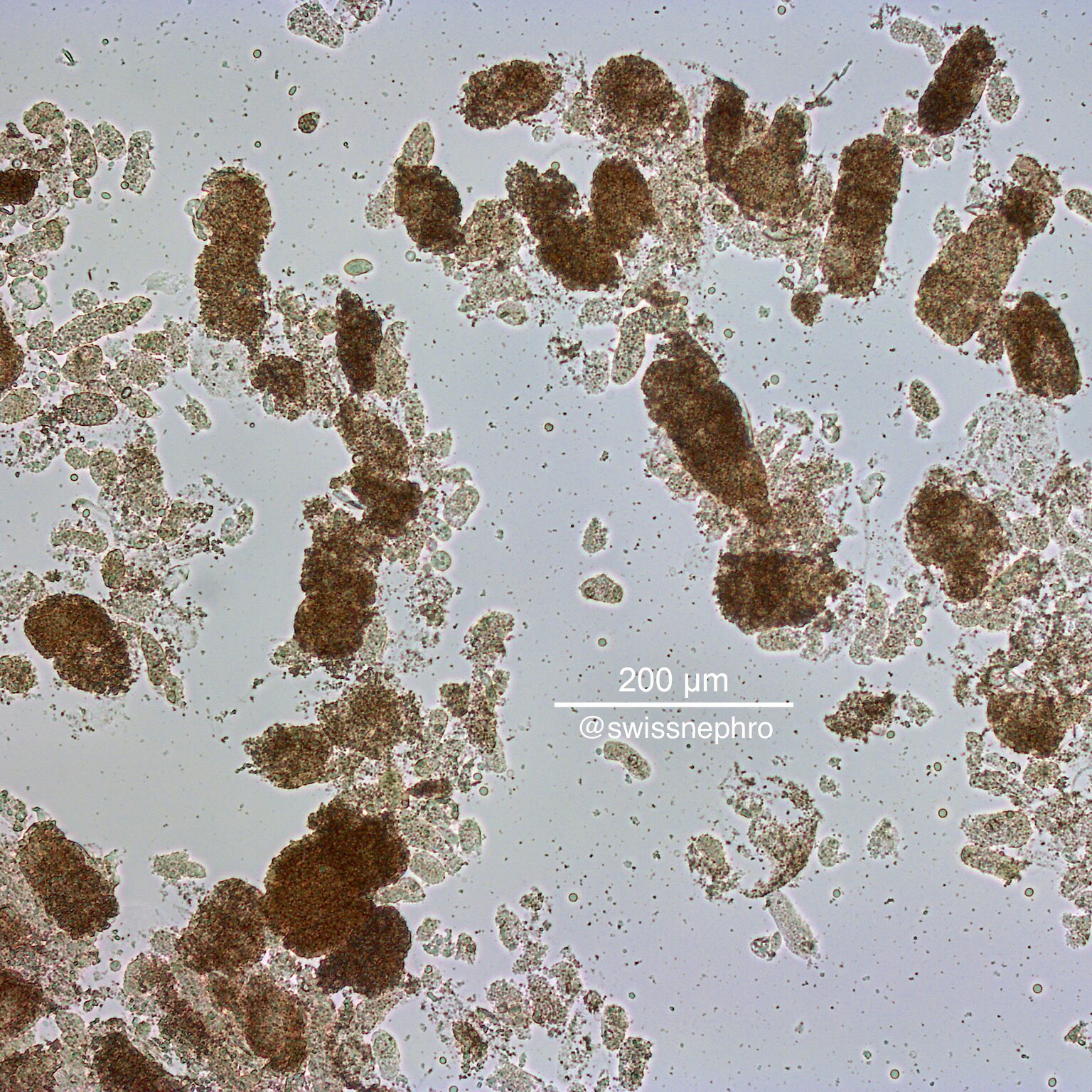
Granular casts
Indicate tubular injury. If dense and brown, they are called “muddy brown casts.” This usually means severe ATN. However granular casts can also be seen in AIN, TMA.

Waxy casts
Indicate severe stasis in the tubules. These are rigid with sharp edges, sometimes with fractures.
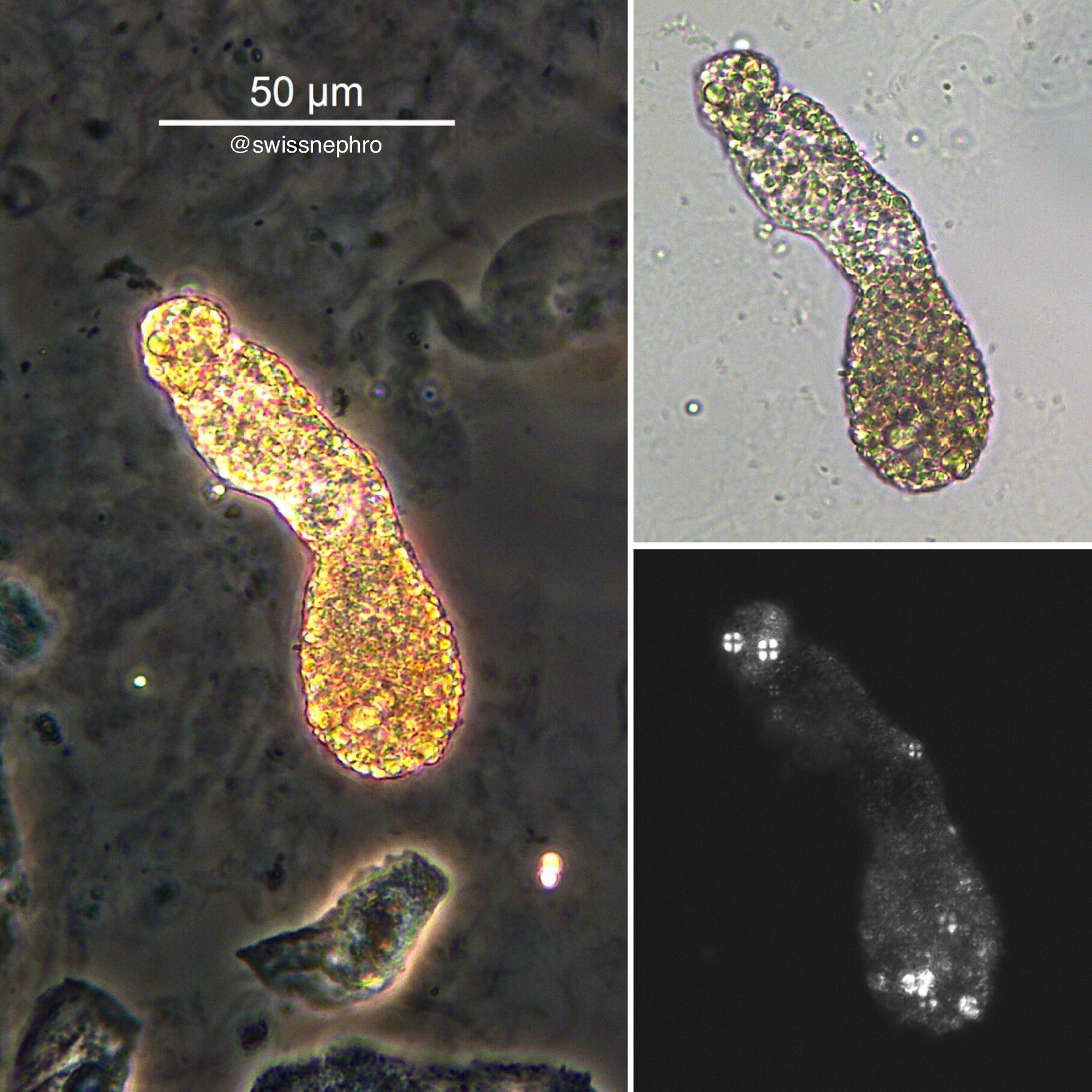
Lipid casts
Indicate nephrotic syndrome. Under polarized light, they look like Maltese cross.
Acute interstitial nephritis
WBC casts are insensitive (<15% in some series) but highly suggestive of AIN in the absence of pyelonephritis.
RTECs, granular casts, and WBCs may also be present in the sediment.
Leukocyturia is variable, however (20-80% of cases). Eosinophiluria is classical but is nonspecific, occurring in other diseases e.g. ATN, GN, DKD.
If concomitant dysmorphic RBCs then consider proliferative GN.
Nephritic syndrome
≥25% dysmorphic RBCs are specific for the patient having any glomerular disease (96%) and glomerulonephritis (90%) but not sensitive (20-30%).
Isomorphic RBCs are often seen in GN too.
Images from Dr. Florian Buchkremer https://twitter.com/swissnephro/media
- Dysmorphic red blood cells https://twitter.com/swissnephro/status/1152258327423979520/photo/1
- Hyaline cast https://twitter.com/swissnephro/status/1095445158836035585/photo/1
- RTEC https://twitter.com/swissnephro/status/1153015089345323008/photo/1
- Granular casts https://twitter.com/swissnephro/status/1150797182783631360/photo/1
- Waxy cast https://twitter.com/swissnephro/status/1041369897660506112/photo/1
- Maltese cross https://twitter.com/swissnephro/status/1114443099529461760/photo/1
MUY DIDACTICO GRACIAS