NEPHROPATHOLOGY
The Pathology of Lupus Nephritis and Lupus Podocytopathy- Part I
A nephropathology session by Dr. Stillman for his presentation. Our Moderator’s Notes are derived from his live presentation.


By Dr. Swati Arora
Key points:
- Up to 50% patients with SLE develop renal disease (>550 mg/ day of proteinuria, and/or active urine sediment) within the first year from SLE diagnosis. But renal disease can present years before or after the development of systemic SLE.
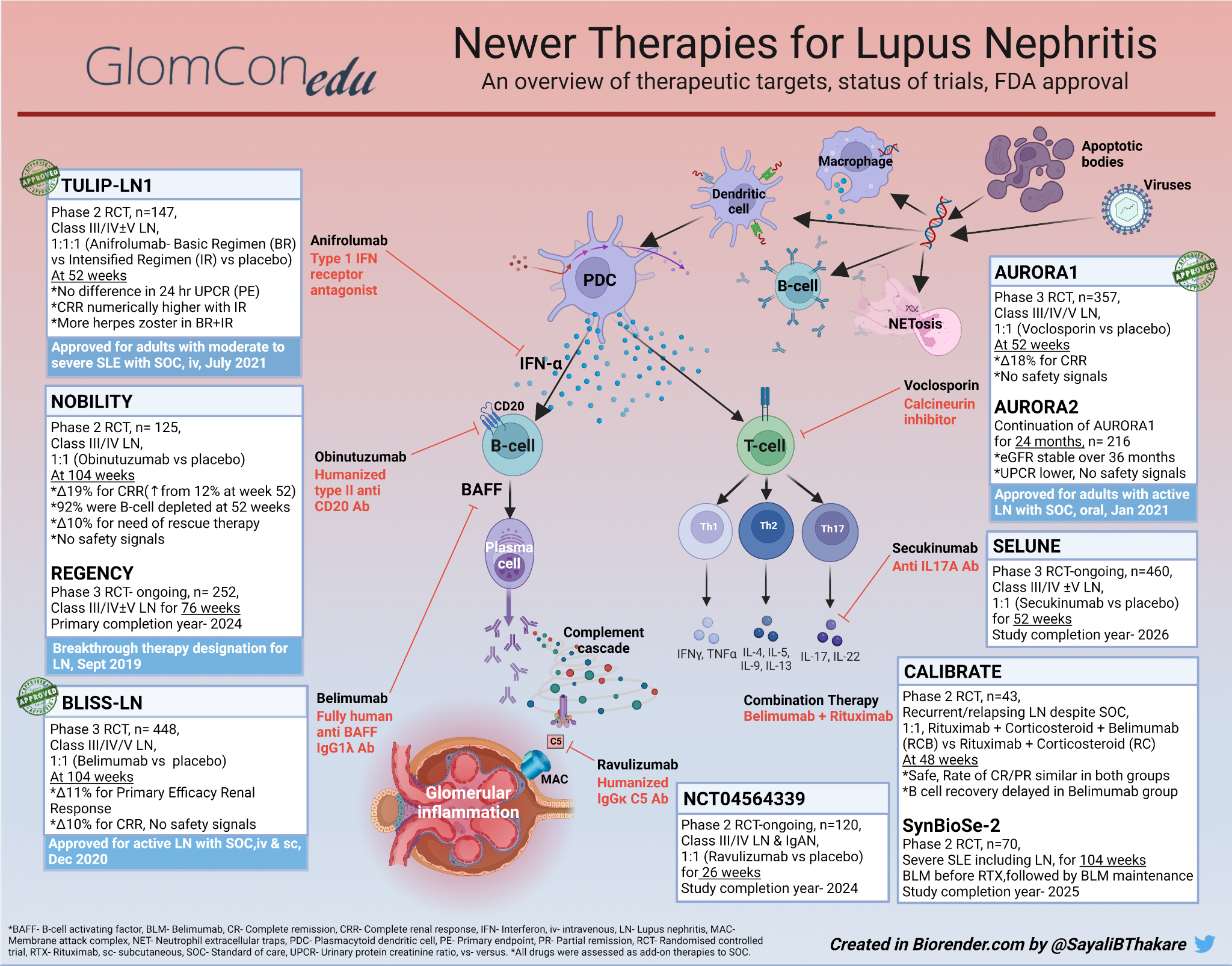
- Lupus nephritis (LN) is defined by the presence of immune deposits by light (LM), immunofluorescence (IF) and/or electron microscopy (EM). The location, nature, and chronicity of the immune deposits primarily determine the type of lesion observed by LM (Class I-VI).
- Other renal lesions lacking immune deposits might also be seen in patients with SLE (e.g. lupus podocytopathy, ANCA overlap, cryoglobulinemic GN, or antiphospholipid antibody associated thrombotic microangiopathy) = lupus-associated renal disease rather than lupus nephritis.
- Immunofluorescence shows full house positive for : C3, C1q, IgG, IgA, IgM.
- Different patterns of injury are as follow:
- Mesangial pattern of injury. Mesangial deposits are hallmark of LN-Clinically: microscopic hematuria, sub-nephrotic proteinuria, normal eGFR-LM: mesangial hypercellularity and proliferation-EM: mesangial EDD, with no cell membrane surrounding them i.e. extra-cellular deposits.
- Epithelial pattern of injury. Clinically: significant proteinuria with nephrotic syndrome, normal to mild decrease in GFR. On LM: Thick GBM spikes (Jones stain). On EM: Discrete subepithelial deposits with varying degrees of lucency (implies chronicity). Over time, intramembranous deposits eventually become lucent and resolve. Also, foot process effacement together with mesangial and sub-endothelial deposits, is strongly suggestive of LN.
- Membrano-proliferative pattern of injury. On LM: Double contours of GBM (outer contour is original GBM, inner contour is new GBM made by endothelial cells, clear space in middle is artifact of staining). On EM: Sub-endothelial deposits.
- Endothelial pattern of injury (Most destructive). Clinical: nephritic , decreased GFR, hematuria, mild to moderate proteinuria. On LM: endocapillary proliferation/ leukocytosis, endothelial injury. On EM: subendothelial immune complex deposits.
- Other findings. Segmental necrosis: Mediated by inflammation. Segmental sclerosis: scarring from prior segmental necrosis. Karryorhectic debris, segmental necrosis, fibrinoid necrosis, leading to cellular crescent, eventually>> fibrocellular>>fibrous crescent.
{kind=link}
{kind=link}
{kind=link}
{kind=link}