GLOMERULAR DISEASE DIAGNOSIS
Urine Microscopy by Dr. Seltzer
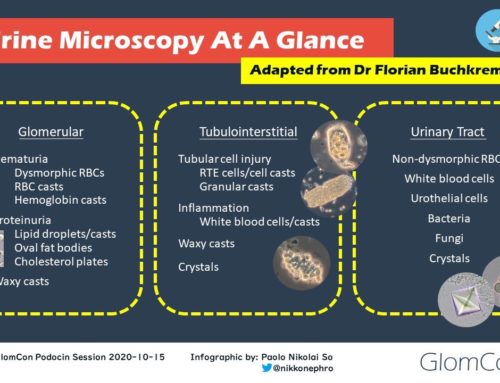
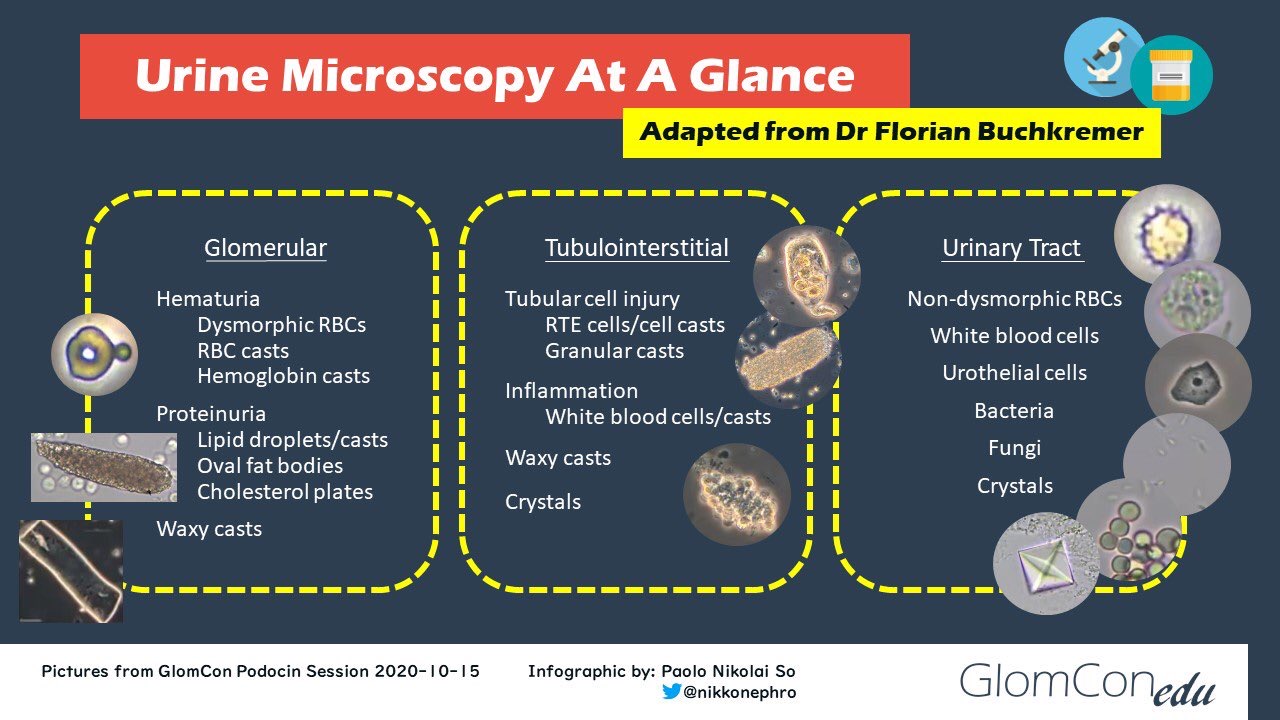
In this session of Nephropathology Essentials, Dr. Seltzer provided a comprehensive review of the art and science of urine microscopy. Our Moderator’s Notes are derived from his live presentation


By Dr. Pravir Baxi
Key points:
- Review of the urinary sediment can (1) provide insight into the etiology of a patient’s acute kidney injury (AKI) and potentially help differentiate between the various causes, (2) help guide the decision to pursue a kidney biopsy and (3) assess the renal response to therapy
- Staining
- Sternheimer-Malbin (SM) stain facilitates identification of WBCs, epithelial cells, and casts
- Sudan III stain (not used routinely) helps identify lipids and is used an adjunct to polarization
- Microscope
- X100, x400 and x1000 magnification options are recommended
- Condenser: focuses the light on a single point in the plane of view; different illumination modalities are changed via the modification of the light coming from the condenser
- Use glass slides and coverslips – not plastic
- Verify proper illumination of the specimen – Kohler Illumination (= a process through which the microscope setup is optimized to provide the best visual quality)
- Produces uniform bright light which focuses on the specimen
- Restricts light exposure of the specimen to the observed field
- Illumination modalities – if available, utilize all four
- Bright Field
- Simplest of all optical microscopy illumination techniques
- Darker sample on a bright background
- Provides the best resolution in a stained specimen
- Dark Field
- Excludes the direct light from the image and thus the field around the specimen is dark
- Helps illuminate unstained or transparent elements against a dark background
- Lower refractive index elements are seen more readily via this modality (such as lipids, crystals, and casts)
- Provides lower resolution than the Bright Field modality
- Phase Contrast
- Enhances contrast of transparent and colorless objects by altering the optical path of light and thus objects will shine out of contrast to adjacent structures
- Good for identifying dysmorphic RBCs
- Polarized Light
- Helps with viewing specimens that are visible primarily due to their optically anisotropic character
- Useful for the identification of lipids, crystals, and contaminants (starch, synthetic fibers)
- Bright Field
- Urine Sediment
- Cells
- Size can help differentiate the type
- Cell diameter: Squamous epi cell > transitional epi cell > renal tubular cell > neutrophil > erythrocyte > bacteria
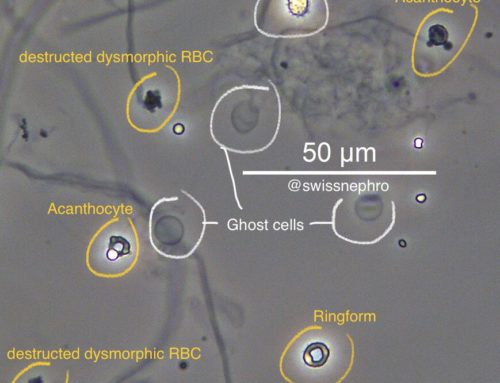
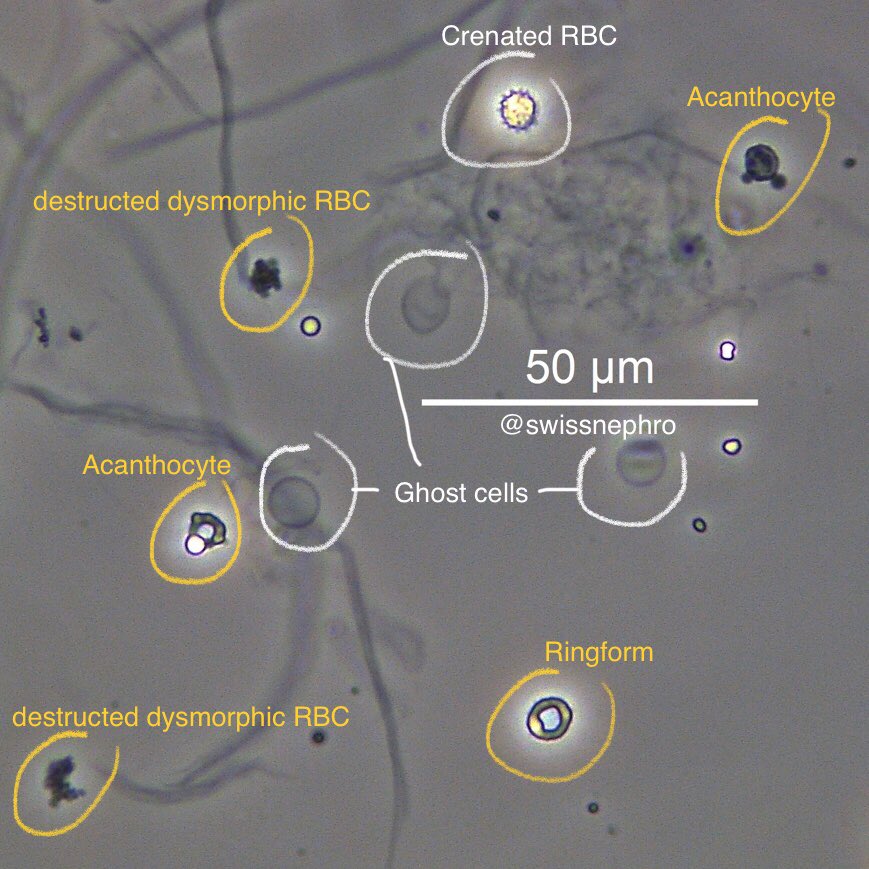
- RBCs
- Normal RBCs will have a round appearance
- Acanthocytes are seen in glomerular hematuria
- Not all dysmorphic RBCs are acanthocytes, and while acanthocytes are considered to be relatively specific for glomerular hematuria, dysmorphic RBCs, in general, are rather non-specific and include crenated RBCs, schistocytes, poikilocytes, etc.
- RBC mimics that may be visible under the microscope: yeast, air bubbles, starch, calcium oxalate, neutrophils, sperm, fat droplets, and pollen
- Neutrophils
- Found in infection and/or inflammation
- These cells have a granular cytoplasm and a segmented multi-lobed nucleus
- The SM stain facilitates visualization of the segmented nucleus
- Glitter Cells – pale staining WBCs with granular motility but these are a non-specific finding
- Size can help differentiate the type
- Lipids
- Oval fat bodies are renal tubular epithelial cells containing fat globules
- They are formed when lipids coalesce into refractile globules on absorption by renal tubular cells
- These oval fat bodies can also be found within a cast
- Sudan III stains are helpful in that it colors the lipids orange
- Oval fat bodies are renal tubular epithelial cells containing fat globules
- Casts
- Formed via solidification of Tamm-Horsfall mucoprotein with other cells/structures within the renal tubules
- Hyaline casts: most common, not pathologic, normal in concentrated urine
- Granular casts
- Can result from the breakdown of cellular casts or degenerative products of tubular cells and proteins
- Classified as fine or coarse, but this has no diagnostic significance
- These are indicative of acute tubular necrosis (ATN)
- Pigmented casts: hemoglobin, myoglobin, bilirubin, and drug pigments
- WBC casts
- Indicative of inflammation or infection
- WBC casts can be present in patients with proliferative glomerulonephritis (GN)
- RBC Casts
- Signify the presence of a proliferative GN or vasculitis process
- Renal Tubular Epithelial casts: indicative of ATN
- Waxy casts: seen in chronic renal failure and thought to represent the end product of cast revolution
- Lipid casts: seen in nephrotic syndrome
- Pseudo-casts: cylindrical appearing structures that resemble a true cast
- Formed when cells or particles adhere to a mucous thread
- Crystals
- Artifacts
- Cells
Selected References:
Fogazzi, G. B., Ponticelli, C., & Ritz, E. (1999). The Urinary Sediment: An Integrated View. Oxford University Press.
Haber, M. H., Blomber, D., Galagan, K., Glassy, E. F., & Ward, P. C. (2010). Color Atlas of the Urinary Sediment: An Illustrated Field Guide Based on Proficiency Testing. College of American Pathologists.
Seltzer, J., Velez, J. C., Buchkremer, F., & Tesser, J. A. (n.d.). Renal Fellow Network (RFN) . Retrieved from https://www.renalfellow.org/category/urine-sediment-of-the-month/
{kind=link}
{kind=link}